Pediatric and adolescent girls
In pediatric and adolescent girls, cardiovascular risk is shaped primarily by congenital anomalies, inflammatory disorders, and drug-related vascular injury (Table 2). Though ACS are rare in this age group, early-life exposures and conditions may establish a foundation for later CVD. Noncoronary cardiac conditions such as hypertrophic cardiomyopathy, long QT syndrome, and inherited arrhythmia syndromes, including Brugada and Wolff-Parkinson-White, are more common than ACS as contributors to sudden cardiac death in this population.
Congenital coronary anomalies
Congenital coronary anomalies are rare and often asymptomatic and diagnosed incidentally, but they can be clinically significant and an important cause of sudden cardiac death among young individuals. Based on angiographic data, prevalence ranges from 0.3 to 1.3% and appears somewhat higher in females69. These anomalies often coexist with structural congenital heart disease (CHD). It is unclear whether the frequency of malignant, interarterial, and intramyocardial course anomalies differs significantly between females and males.
Children born with CHD who survive into adulthood are at increased risk of premature CAD, likely due to interactions between congenital alterations, cumulative endothelial dysfunction, and traditional risk factors69,70. Some data suggest that women born with CHD may be at higher risk for CAD than males with CHD, speculated to be due to lower rates of traditional risk factors like smoking or hyperlipidemia in men with CHD when compared to women71. This potential shift in risk burden requires further study, as current data are limited.
Inflammatory and autoimmune disorders
Kawasaki disease is the most common cause of acquired heart disease in children in developed countries, with an annual U.S. incidence of 20–25 per 100,00072. Kawasaki is male-predominant, but long-term sequelae in females may still contribute to early CAD.
In contrast, SLE is strongly female-predominant, and pediatric-onset SLE carries a high risk for premature CAD, even in the absence of traditional risk factors73,74. This excess risk is attributed to chronic inflammation, cytokine dysregulation, oxidative stress, antiphospholipid antibodies, and vascular toxicity from immunosuppressive therapies75. Juvenile idiopathic arthritis also affects girls disproportionately and has been associated with increased arterial stiffness and subclinical atherosclerosis76. Additionally, childhood cancer survivors, including girls treated for Hodgkin lymphoma with mantle radiation, face increased long-term risk of CAD, valvular disease, and cardiomyopathy77. Despite this, there is no validated cardiac risk assessment strategy for pediatric SLE, arthritis, or cancer survivors, and limited consensus on screening or prevention, posing challenges for early intervention.
Medication and illicit substance-related vascular injury
Among adolescents, vascular dysfunction from medications or substances is an emerging concern. Prescription stimulants (e.g., for attention-deficit hyperactivity disorder) are widely used in adolescent populations. While generally safe, high doses or prolonged use have been associated with elevated blood pressure and increased arterial stiffness, particularly in those with predisposing risk factors78. Sex-specific surveillance data are limited, and it remains unclear whether cardiovascular effects differ between girls and boys.
Beyond prescription stimulants, other substances increasingly used by adolescents may contribute to vascular dysfunction and elevated cardiovascular risk. Epidemiological data demonstrate that recreational substance use (e.g., tobacco, alcohol, cocaine, amphetamines, cannabis) is independently associated with premature and extremely premature atherosclerotic CVD, and the magnitude of risk is greater among women than men79. Cannabis smoking, vaping, or ingestion, while often perceived as benign, has been associated with coronary vasospasm, arrhythmias, and increased myocardial oxygen demand, particularly when combined with tobacco or stimulants80. These effects are not sex-specific, but the epidemiological evidence indicates that the adverse cardiovascular impact may be more pronounced in women81.
Cocaine is clearly linked to ACS risk via coronary vasospasm, endothelial injury, and prothrombotic effects82. Women with cocaine use disorder have a significantly higher risk of cardiovascular hospitalization when compared to women who do not use cocaine, though these data largely reflect adult populations83. Methamphetamines, though less common in younger teens, are strongly linked to ACS via catecholamine surge and vasoconstriction79. High-caffeine energy drinks, popular among adolescents, may exacerbate hypertension and trigger arrhythmias or QTc prolongation, especially when consumed in excess or with physical exertion84. These exposures are often underrecognized in clinical assessment but may contribute to early vascular injury and should be considered in cardiovascular risk screening.
E-cigarette use has grown rapidly among adolescent girls. While long-term outcome data are lacking, early studies show associations with increased blood pressure, vascular stiffness, arrhythmias, and endothelial dysfunction85. The AHA has emphasized concern about cardiopulmonary consequences and has called for more longitudinal data to assess cardiovascular outcomes in youth86.
Reproductive-age women (20s–40s)
Cardiovascular disease in reproductive-age women is often underrecognized and misattributed, despite increasing evidence of unique pathophysiologic mechanisms, sex-specific risk factors, and distinct clinical presentations2.
Atherothrombosis
Atherothrombosis remains the leading cause of MI, even in reproductive-age women (Fig. 2). There is evidence of both a rising burden of atherothrombotic events and CVD mortality in middle-aged women and distinct mechanisms compared to men3. Coronary thrombosis occurs via plaque rupture, plaque erosion, or calcific nodules. Plaque rupture accounts for ~80% of fatal MIs in men but only ~60% in women87. Plaque erosion appears more common in women, particularly younger and premenopausal women, suggesting a possible protective role of estrogen against plaque rupture (which is uncommon in young women)88. Notably, a history of preeclampsia has been associated with increased CVD risk and a specific predisposition toward plaque erosion89.

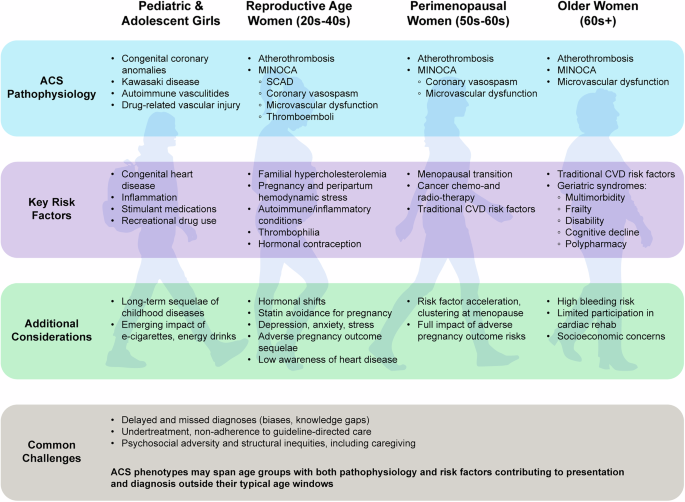
Women experience acute coronary syndrome (ACS) through both obstructive and non-obstructive mechanisms, with notable age-based variability. Atherothrombotic causes such as plaque rupture, erosion, and calcific nodules predominate in postmenopausal and older women, while non-obstructive causes, including spontaneous coronary artery dissection (SCAD), coronary vasospasm, microvascular dysfunction, and coronary embolism, are disproportionately represented in women under age 60. Mechanisms may coexist or evolve across the lifespan. MINOCA myocardial infarction with non-obstructive coronary arteries.
Familial hypercholesterolemia (FH) is a major driver of early-onset CAD in women. Among those with an FH phenotype, women tend to experience earlier onset of ASCVD than men, with risk accelerated by 20–30 years90. Delayed diagnosis and treatment, along with pregnancy-related interruptions in statin therapy, contribute to worse outcomes91. Women with untreated FH face a 10–20-fold higher ASCVD risk and up to 30% chance of MI before age 6092.
Myocardial infarction with non-obstructive coronary arteries (MINOCA)
Myocardial infarction with non-obstructive coronary arteries (MINOCA) is a heterogeneous clinical syndrome occurring in approximately 5-15% of patients presenting with acute MI, more frequently in women6. By definition, MINOCA involves evidence of MI with no obstructive CAD (<50% stenosis) on angiography. Pathophysiologic mechanisms include plaque disruption with distal embolization, coronary vasospasm, SCAD, coronary microvascular dysfunction, and coronary thromboembolism. Sex-specific factors, including endothelial dysfunction, hormonal influences, and differential vascular responses, may contribute to the higher prevalence of MINOCA in women. Accurate diagnosis requires exclusion of alternate non-ischemic causes of troponin elevation (e.g., myocarditis, Takotsubo syndrome, arrhythmias) and often relies on adjunctive testing such as intracoronary imaging and especially early cardiac MRI93,94. In a community cohort retrospectively utilizing all clinical data among patients with troponin elevation, including coronary angiography, the rate of truly unclassifiable MINOCA in women aged 65 or younger was only 3%7.
Spontaneous coronary artery dissection
SCAD occurs disproportionately in women (85–90% of cases), and while it accounts for a minority of ACS overall, approximately 10% of MIs in women under age 65, up to a quarter under age 55, and 40% of pregnancy-associated MI cases are due to SCAD, highlighting its disproportionate impact in these populations4,7,95. SCAD results from an intramural hematoma or intimal tear that separates arterial wall layers, causing luminal compression or an obstructing flap. The identification and diagnosis of SCAD by coronary angiography can be overlooked when only subtle evidence is seen. Increasing awareness of this entity, particularly in young women, and intracoronary imaging such as intravascular ultrasound (IVUS) or optical coherence tomography (OCT) have increased recognition in ACS patients4.
SCAD4 is associated with several non-atherosclerotic arteriopathies, including fibromuscular dysplasia (present in 40–80% of cases), coronary artery tortuosity, and, rarely, connective tissue disorders like Marfan or Ehlers-Danlos syndromes (seen in up to 5% of cases)96. Pregnancy-associated SCAD is often more severe, with multivessel or left main involvement96. Hormonal influences have been hypothesized, but the occurrence of SCAD in nulliparous and postmenopausal women suggests multifactorial mechanisms. Triggers are noted in up to 25% of patients and include extreme physical exertion and Valsalva-like maneuvers (e.g., retching, coughing), and emotional stress97.
ACS due to coronary artery emboli
Embolic MI is also uncommon (2–5% of ACS cases), but important in younger women due to the frequent use of systemic hormonal contraceptives, which can predispose to thrombus formation98. Atrial fibrillation is the most common cause of coronary embolus overall, but other contributors include cardiomyopathies, prosthetic valve dysfunction, infective endocarditis, hypercoagulable states (de novo arterial thrombi and venous thrombi with paradoxical embolization), and cardiac tumors such as papillary fibroelastomas (PFE)98. These disorders should be considered in young women with MI in the absence of obstructive disease at coronary angiography52. Embolic MI is associated with higher morbidity and mortality, including increased risk of recurrent thromboembolism, MACE, and early mortality, especially in the context of atrial fibrillation99,100. Women with embolic MI may present at a younger age and with fewer traditional risk factors52. Prompt recognition and systematic evaluation for embolic sources are critical for appropriate management and secondary prevention. If paradoxical embolization is on the differential, evaluation to rule out an intracardiac shunt, including a patent foramen ovale, should be performed, with closure if clinically relevant.
Thrombophilia affects men and women equally, but hormonal states (pregnancy, oral contraceptives, hormone therapy) amplify thrombotic risk in women101. An inherited thrombophilia (e.g., factor V Leiden, prothrombin G20210A) confers a higher odds ratio for acute MI in young women compared to men102. Antiphospholipid syndrome, more common in women, confers particularly high thrombotic risk103.
PFEs are more frequently found in women, with large surgical and echocardiographic series consistently reporting a female predominance of over 60%104. While the primary clinical risk of PFEs is embolic stroke, embolic MI rarely occurs, typically in the context of left-sided, mobile, or aortic valve PFEs104.
Coronary vasospasm and microvascular dysfunction
Coronary vasospasm and microvascular dysfunction are closely linked and disproportionately affect women, especially those with MINOCA or INOCA29. It is estimated that 30–50% of patients with INOCA have microvascular dysfunction, especially women under 50 years of age6. In the WISE study, nearly two-thirds of women with MINOCA as the cause of ACS had microvascular dysfunction identified on stress cardiac magnetic resonance imaging, and up to one-third of women with non-obstructive CAD had vasospasm detected by acetylcholine provocation testing105,106. These entities contribute significantly to angina and ischemia in young women and are often underdiagnosed.
Importantly, microvascular dysfunction can be both a cause and a consequence of ischemia, which complicates risk stratification. It is also highly prevalent and associated with a worse prognosis among women with heart failure with preserved ejection fraction107. These mechanisms highlight the need for advanced diagnostic evaluation and sex-specific management strategies.
Peripartum and pregnancy-associated ACS
Cardiovascular disease is the leading cause of pregnancy-associated mortality in the United States, with ACS representing a growing proportion of these events. The risk of MI increases 3-fold during the peripartum period, with the highest incidence in the third trimester and early postpartum108. The incidence of pregnancy-associated MI is estimated at 2.8–8.1 per 100,000 deliveries, with maternal mortality rates ranging from 4.5 to 7.3%109.
According to a recent population-based study, most pregnancy-associated ACS are non-atherosclerotic in origin. SCAD is the most common mechanism, accounting for up to 44% of cases110. Other etiologies include atherosclerosis, coronary embolism, coronary thrombosis (often without underlying plaque), and coronary vasospasm. Sometimes, the coronary arteries appear normal on imaging, such that the etiology is uncertain. The hypercoagulable state of pregnancy, characterized by increased procoagulant factors, reduced fibrinolysis, and acquired protein C resistance, further contributes to thrombotic risk108. These changes are hormonally mediated, present early in gestation, and persist postpartum.
Hypertensive disorders of pregnancy, particularly preeclampsia and HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome, are common CVD risk enhancers111,112. Preeclampsia is associated with a 71% increase in cardiovascular mortality and a two- to four-fold increase in long-term CAD, heart failure, and stroke112. These outcomes are mediated in part by the subsequent development of chronic hypertension, diabetes, and dyslipidemia111. Low-dose aspirin is recommended in high-risk pregnancies to reduce preeclampsia risk113. Additional prevention strategies include lifestyle changes targeting regular exercise, smoking cessation, and balanced dietary intake114. Importantly, Black women in the U.S. are disproportionately affected by hypertensive pregnancy disorders and peripartum cardiovascular complications22. Biological factors, such as genetic variants, may also contribute to this increased risk, in addition to systemic inequities and healthcare disparities.
Women with prior ACS, whether due to atherosclerosis, SCAD, or other causes, are considered high risk for subsequent pregnancy-related cardiovascular events. Women with prior MI should be counseled that pregnancy may require medication adjustment and, in itself pose increased risk, especially in the early postpartum period4,101,115. Shared decision-making, ideally within a multidisciplinary cardio-obstetrics team, is critical to determine whether and when pregnancy is advisable. For instance, DAPT can be associated with increased maternal and fetal bleeding101. In most cases, it is recommended to complete the necessary DAPT course prior to conception. If pregnancy occurs while on DAPT, decisions must be individualized in consultation with cardiology, maternal-fetal medicine, and hematology specialists. Aspirin is generally considered safe in pregnancy and may be continued. The decision to continue or modify DAPT should be made on a case-by-case basis, balancing maternal cardiovascular risk and fetal safety, and planning for delivery and anesthesia115.
Contraception and hormone therapy
Combined hormonal contraceptives (CHCs) increase the risk of venous thromboembolism (VTE) by seven- to eight-fold, with risk varying by estrogen dose and progestin formulation116. Since non-oral systemic hormonal formulations bypass first-pass metabolism of the liver, avoiding the activation of clotting factors, triglycerides, and inflammatory markers, as seen with oral estrogen, these have been considered a safer option. However, some reports have shown non-oral formulations confer similar risk, perhaps by other mechanisms117. Progestin-only contraceptives (POCs), such as the levonorgestrel intrauterine device (IUD) or progestin-only pills, do not increase VTE risk, with the exception of injectable medroxyprogesterone acetate, which may have a modest effect118. IUDs, including copper and levonorgestrel-releasing types, do not increase cardiovascular risk and are considered safe for women with or at risk for cardiovascular disease, including those on anticoagulation119.
Women with antiphospholipid syndrome, SLE, or inherited thrombophilia should avoid CHCs. In these cases, POCs or non-hormonal methods are preferred, as supported by the American College of Radiology and ACC/AHA consensus120.
Peri- and early postmenopausal women (50s–60s)
The perimenopausal and early postmenopausal years represent a pivotal stage in the emergence of ischemic heart disease in women. This period is marked not only by increasing cardiovascular risk but also by changing disease patterns and diagnostic challenges. For instance, the use of systemic menopausal hormone therapy (MHT) can increase the risk of VTE, stroke, and possibly coronary events. As such, MHT is not routinely recommended for the primary or secondary prevention of CVD. However, when initiated in healthy women younger than 60 years or within 10 years of menopause onset, MHT appears to be associated with low CV risk and may confer cardiometabolic benefits121. In contrast, MHT initiation later in life or in women with established atherosclerosis is associated with greater adverse cardiovascular outcomes. Risk stratification based on age, time since menopause, and comorbidities is essential. Nonsystemic, topical MHT, such as vaginal estrogen do not have systemic effects and is safe to use, especially for genitourinary symptoms122. For many women, this is also a life stage that may include changing demands at work, musculoskeletal issues, and associated decreased exercise, or new caregiving responsibilities for aging parents, all of which may adversely affect cardiovascular health and contribute to the upward inflection of cardiovascular risk factors, particularly decreased physical activity, weight gain, and increasing blood pressure.
Atherosclerotic ACS
Compared with men, women in this age group experience a delayed onset of obstructive ACS, on average, a decade later, but the delay is paralleled by a lag in recognition and diagnosis. Clinical presentation may be subtle, with symptoms such as exertional fatigue, nausea, sleep disturbance, or dyspnea being more prominent than chest pain. These patterns contribute to diagnostic uncertainty, delayed triage, and lower rates of guideline-based therapies at presentation11,14.
Menopause, the clinical and risk factor inflection point
Many women first develop overt coronary symptoms or events during the menopausal stage. The menopause transition is associated with adverse changes in lipids, body fat distribution, and vascular function, which accelerate cardiovascular risk and often coincide with the initial presentation of coronary symptoms in women aged 50–60 years26.
A substantial proportion of women in this age group have angina with normal or minimally diseased epicardial coronary arteries123. These women are at increased risk for adverse outcomes, including recurrent hospitalizations and higher mortality, underscoring that angina and/or ischemia without obstructive disease is not benign123. Clinicians should maintain a high index of suspicion for ischemic heart disease in symptomatic menopausal women, even in the absence of obstructive epicardial disease, and pursue appropriate diagnostic and management strategies14.
Non-obstructive ACS
Women in their 50s and early 60s are disproportionately affected by MINOCA, which accounts for approximately 6–15% of all MI presentations in women, with higher prevalence compared to men6. Common mechanisms include plaque erosion, SCAD, vasospasm, and thromboembolism, discussed above. Microvascular dysfunction, a leading cause of exertional chest pain and reduced quality of life in middle age in older women, may rarely cause ACS, but most often presents with exertional angina, abnormal stress testing, and normal or near-normal coronary imaging45. These etiologies may be missed or miscategorized with coronary angiography alone, necessitating advanced intracoronary imaging such as optical coherence tomography (OCT) or intravascular ultrasound (IVUS) and early cardiac magnetic resonance (CMR) to clarify the underlying cause94,124.
Older women (60s+)
In later life, the burden of atherosclerotic CVD becomes increasingly pronounced in women. However, the clinical expression of ACS in older women often diverges from textbook paradigms, with important implications for recognition, management, and outcomes.
Atherosclerotic ACS in the setting of multimorbidity
Atherosclerotic ACS is the predominant phenotype in women over age 60, often occurring in the setting of multiple comorbidities such as hypertension, diabetes, chronic kidney disease, and anemia. These coexisting conditions contribute to atypical presentations, higher procedural risk, and more complex medical management when compared to younger individuals125. Despite similar plaque burden compared to men, older women are less likely to undergo early invasive evaluation or receive guideline-directed medical therapy at discharge, even when presenting with high-risk features125. Provider bias, both conscious and unconscious, also plays a significant role, as clinicians are less likely to recommend invasive evaluation for women, even when clinical vignettes are identical to those of men126. Contemporary registry data also suggest that sex differences can extend into the post discharge period; in the PRAISE registry, women had different post discharge clinical profiles and outcomes compared with men, with differences attenuated after multivariable adjustment127.
When revascularization is pursued, women have higher rates of vascular complications and bleeding. This is attributed to smaller vessel caliber, older age, higher prevalence of anemia and renal dysfunction, and increased sensitivity to antithrombotic agents128. Women may derive a relatively greater absolute benefit from radial access in the setting of increased vascular access complications; however, the guideline recommendations to prioritize radial access are not sex specific129,130. Furthermore, women have smaller coronary arteries, which present additional technical challenges during PCI and may impact long term results131. Older women may also derive less symptomatic benefit from PCI in the presence of diffuse or microvascular disease, which is more prevalent in this patient population group131.
Under-recognition of symptoms
Women who are 75 or older more frequently present with multiple and less obvious ischemic symptoms, including weakness, confusion, nausea, or falls, rather than chest pain128. This symptom profile, coupled with age- and gender-based biases, contributes to diagnostic delay and lower likelihood of receiving reperfusion therapy in ST-elevation ACS128. Cognitive impairment, sensory limitations, and social isolation further complicate symptom recognition and timely presentation125.
Frailty, disability, and polypharmacy
Frailty, defined as reduced physiologic reserve and increased vulnerability to stressors, affects a substantial proportion of older women with ACS and is independently associated with higher mortality, bleeding, and poor functional recovery125,132. Disability, both pre-existing and acquired post-ACS, further complicates recovery, limits participation in cardiac rehabilitation, and increases the risk of long-term institutionalization125. Polypharmacy, common in this population, raises the risk for adverse drug interactions, medication non-adherence, and cognitive side effects125. Importantly, clinical trial data guiding ACS therapy in frail, disabled older adults, particularly women, are limited, necessitating individualized, goal-aligned care that balances longevity with functional outcomes and quality of life. Patient-centered approaches are essential in this population, ensuring that treatment decisions align with individual goals, preferences, and functional priorities, particularly in the context of multimorbidity and age-related complexity133.
Consideration for antiplatelet therapy after ACS in women
Sex-specific considerations are critical in the use of DAPT for women with ACS, particularly those of reproductive age. Women have a higher prevalence of non-atherothrombotic ACS mechanisms and are at greater risk for bleeding complications, including menorrhagia and peripartum hemorrhage134. Sex-specific data on DAPT duration and selection are limited, especially in patients with MINOCA, SCAD, and cancer- or autoimmune-related ACS, where pathophysiology may not require prolonged platelet inhibition. A 2025 clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions and the ESC Working Group on Thrombosis identifies strategies to improve the safety and efficacy of antithrombotics in women with ACS. The authors highlight the underrepresentation of women and sex-based analyses in current research and emphasize the importance of including women in randomized controlled trials so that sex-based analyses and recommendations can be sufficiently performed130.
In women with SCAD, conservative management is preferred in clinically stable patients, given the high rate of spontaneous healing and the elevated procedural risks associated with PCI4. Once SCAD is confirmed, anticoagulation initiated for ACS is usually discontinued unless otherwise indicated. For those managed without revascularization, antiplatelet therapy practices vary and are an active area of investigation. While single antiplatelet therapy with aspirin is commonly used, the optimal regimen and duration remain unproven. Observational data suggest that DAPT, especially with more potent P2Y12 inhibitors, may be associated with a higher risk of early adverse events in conservatively managed SCAD, supporting individualized, often restrained use of DAPT in this context135,136. In contrast, when PCI is performed for SCAD, DAPT is indicated; however, duration should be tailored to bleeding risk and coexisting atherosclerosis130. In select patients, shorter DAPT (1–3 months) followed by P2Y12 monotherapy may be reasonable, though evidence is extrapolated from non-SCAD PCI trials. Similarly, the role of DAPT in MINOCA and INOCA remains poorly defined and should be tailored to the suspected mechanism6,130.
Cardiac rehabilitation in women across the lifespan
Cardiac rehabilitation (CR) is a Class I recommendation endorsed by the AHA, ACC, and partnering societies for all eligible patients following ACS126,137. Despite these benefits, women remain underrepresented in every stage and every age of CR utilization, especially among very elderly and reproductive age women. Sociocultural and structural factors compound these gaps. Women are more likely to serve as primary caregivers and may prioritize the health of others over their own. Financial constraints, limited insurance coverage, and logistical challenges such as transportation or time off work reduce participation. Women of lower socioeconomic status and those without insurance are significantly less likely to attend CR; insured patients are three times more likely to be referred.
A recent multi-society endorsed AHA scientific statement emphasizes that CR improves women’s functional status, reduces hospital readmissions, lowers mortality, and enhances quality of life. The authors emphasize the need to improve referral and participation among women and to provide gender and culturally sensitive CR programming that is tailored to the individual woman’s unique physiological, psychological, and social needs, as well as ACS diagnosis. Improving the effectiveness and participation of CR will require employing non-traditional models that emphasize mental health, address sex differences in physiology, and gender differences in priorities, and for clinicians to emphasize its importance to their patients.

